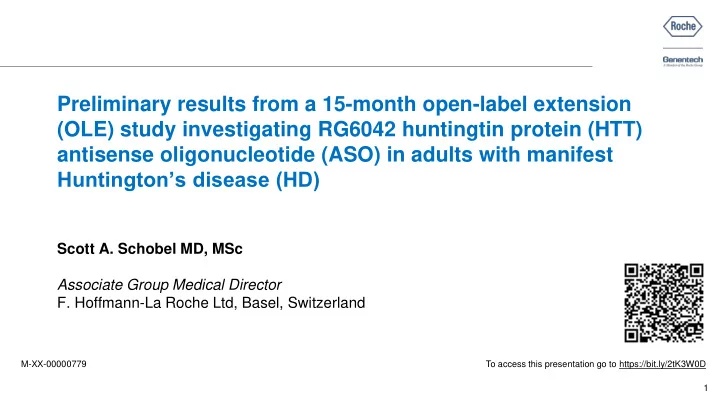
SLIDE 25 Simulation of Q8W and Q16W dosing to achieve pharmacologically relevant effect (120 mg IT) Month mHTT change from baseline (%) –20 –40 6 12 18 21 24 3 15 9
–44%
mHTT % change at trough at steady-state 120 mg Q8W
A clinical population PK/PD model based on Phase I/IIa and OLE data supports programme shift to less frequent dosing
* Q4W dose was verified with VPC and goodness-of-fit plots before simulating Q8W and Q16W.
† Table based on preclinical data.
CSF, cerebrospinal fluid; IT, intrathecal; KD, knockdown; mHTT, mutant huntingtin protein; OLE, open-label extension; PD, pharmacodynamic; PK, pharmacokinetic; popPK/PD, population PK/PD; Q8W, every 2 months; Q16W, every 4 months; VPC, visual predictive check. Sanwald Ducray P, et al. Neurology. 2019; 92(15 Suppl):S16.005.
25
Observed mHTT data (9 months) Observed mHTT data (15 months) Median popPK/PD model predictions 120 mg IT Q8W 25–75% prediction interval 120 mg IT Q8W popPK/PD model predictions 120 mg IT Q16W 25–75% prediction interval 120 mg IT Q16W
120 mg Q8W exceeds trough CSF mHTT preclinical efficacy threshold in cortex and caudate; 120 mg Q16W in cortex only GENERATION HD1 pivotal study dose regimen changed from Q4W/Q8W to Q8W/Q16W –25%
mHTT % change at trough at steady-state 120 mg Q16W Estimated acute lowering ~35%
% CSF HTT KD† % HTT KD in cortex % HTT KD in caudate 20–30 30–55 5–20 30–40 40–70 15–35 40–50 55–80 25–45
Phase I/IIa and OLE data used to develop PK/PD model (120 mg IT Q8W)* Month mHTT change from baseline (%) –40 –20 –80 –60 6 12 18 21 24 3 15 9
Empirical trough pre-dose CSF data