SLIDE 34 Introduction The 2 existing approaches How we fit fully-parametric model Illustration Discussion Summary
10 15 20 25 −6.0 −5.6 −5.2 −4.8
intercept sample
- ● ● ●
- ● ●
- ● ● ●
- ● ● ● ● ● ●
5 10 15 20 25 0.02 0.04 0.06
age sample
10 15 20 25 0.0 0.2 0.4
male sample
- ● ● ● ●
- ● ●
- ● ● ● ● ● ● ● ● ● ● ● ●
5 10 15 20 25 0.0 0.2 0.4 0.6
black sample
- ● ● ● ●
- ● ●
- ● ● ●
- ●
- ● ● ● ● ● ● ●
- 5
10 15 20 25 0.005 0.015 0.025
sbp sample
- ● ● ● ●
- ●
- ● ● ●
- ● ●
- ●
- ●
- ● ● ● ●
5 10 15 20 25 −0.8 −0.4 0.0 0.4
tx sample
- ● ●
- ● ●
- ● ● ●
- ●
- ●
- ● ● ● ● ●
- ● ●
5 10 15 20 25 −0.15 −0.05 0.05
t sample
- ● ● ● ● ●
- ● ● ●
- ● ●
- ● ●
- ●
- ●
- ● ●
5 10 15 20 25 −0.3 −0.1 0.0 0.1
tx*t sample
- ● ●
- ● ● ● ●
- ● ● ● ● ● ● ● ● ● ● ● ●
- 5
10 15 20 25 0.10 0.15 0.20
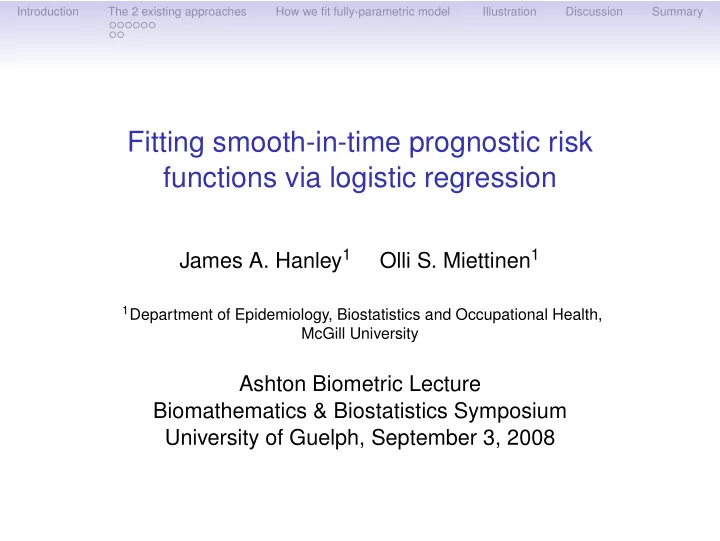
5 year Risk sample
STABILITY ?
Point and (95% confidence) interval estimates of hazard function, and of 5-year risk for a specific (untreated) high-risk
- profile. Fits are based
- n 25 different random
samples of b =26,300 from the infinite number of person-moments in the study base, and same c = 263 cases each run.