
SLIDE 1
GCIG Education Symposium, November 2017, Vienna
f
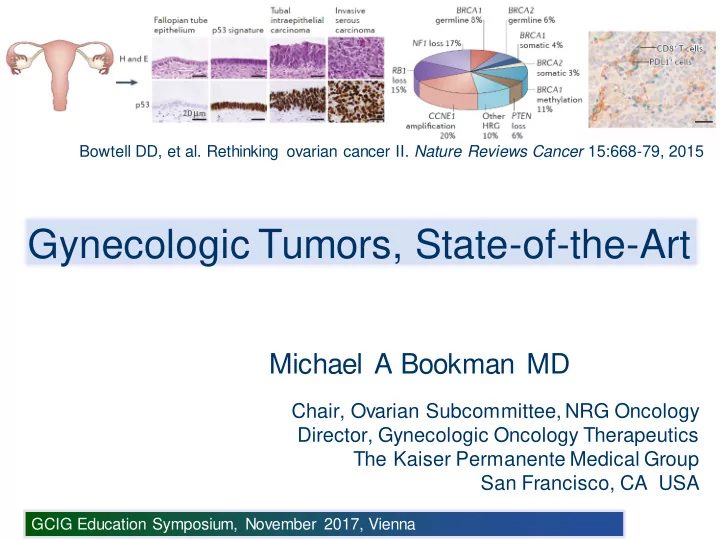
Bowtell DD, et al. Rethinking ovarian cancer II. Nature Reviews Cancer 15:668-79, 2015
Gynecologic Tumors, State-of-the-Art Michael A Bookman MD Chair, - - PowerPoint PPT Presentation
f Bowtell DD, et al. Rethinking ovarian cancer II. Nature Reviews Cancer 15:668-79, 2015 Gynecologic Tumors, State-of-the-Art Michael A Bookman MD Chair, Ovarian Subcommittee, NRG Oncology Director, Gynecologic Oncology Therapeutics The Kaiser
GCIG Education Symposium, November 2017, Vienna
Bowtell DD, et al. Rethinking ovarian cancer II. Nature Reviews Cancer 15:668-79, 2015
GCIG Education Symposium, November 2017, Vienna
Ferlay J, et al. GLOBOCAN 2008 v2.0: International Agency for Research on Cancer
GCIG Education Symposium, November 2017, Vienna
GCIG Education Symposium, November 2017, Vienna
Woodman BJ, et al. Nature Rev Cancer 2007; 7:11-22
GCIG Education Symposium, November 2017, Vienna
Doorbar J, et al. Vaccine 2012;30S:F55-70 Predominance of E6 and E7 with loss of capsid proteins (L1 and L2)
GCIG Education Symposium, November 2017, Vienna
? Neoadjuvant Chemotherapy Clinical Staging ? Fertility-Sparing or Risk-Stratified Surgery ? Adjuvant ChemoRx ? Vaginal BrachyRT Recurrence Chemotherapy +/- anti-VEGF Cellular Immunity Vaccines Immune Checkpoint Inhibition Surgery Alone Radiation +/- Concurrent Chemotherapy ? Dose- Schedule
GCIG Education Symposium, November 2017, Vienna
Plante M for NCIC CTG and GCIG-CCRN
*Includes PLD (optional SLN) Low-Risk Cervical Cancer:
stroma, <50% stromal invasion
Stratified by Centers (SLN yes/no), Stage, Histology, Grade Post-operative adjuvant therapy permitted based on final pathology Primary Endpoint: Pelvic Relapse-Free Survival (PRFS) Non-inferiority design, p = 0.05, 80% power with one interim analysis Open: 01-DEC-2012 Target: 700 pts
GCIG Education Symposium, November 2017, Vienna
McCormack M for CRUK-NCRI and GCIG-CCRN Carboplatin AUC=2 Paclitaxel 80 mg/m2 (Weeks 1-6) Standard CRT*
*40 to 50.4 Gy + weekly Cisplatin + ICBT
Stratified by Stage, LN status, Histology, T volume, Institution, IRMT (Yes/No) Primary Endpoint: Overall Survival p = 0.05, 80% power to detect a 10% increase in 5 year OS Open: NOV-2012 Target: 630 pts Standard CRT*
GCIG Education Symposium, November 2017, Vienna
Meta Analysis Collab. J Clin Oncol 26:5802-5812, 2008
GCIG Education Symposium, November 2017, Vienna
Ryu for KGOG-ASGO and GCIG-CCRN Radiation Therapy with Cisplatin 40 mg/m2 (Weekly x6) Radiation Therapy with Cisplatin 75 mg/m2 (Tri-Weekly x3)
Primary Endpoint: Overall Survival p = 0.05, 80% power to detect a 10% increase in 5 year OS, HR = 1.50 Open: MAR-2012 Target: 590 pts
ICBT ICBT
GCIG Education Symposium, November 2017, Vienna
Mileshkin L (ANZGOG), Moore K (NRG), et al. In progress Carboplatin AUC=5 Paclitaxel 155 mg/m2 (3 h) x4
R I II Concurrent Chemo-Radiation Cisplatin 40 mg/m2/wk + Intracavitary Brachytherapy Observation Open: 03-JAN-2012 Closed: 28-JUN-2017 (5.5 y) Accrual: 780 pts (increased to 900)
GCIG Education Symposium, November 2017, Vienna
Tewari KS, et al. NEJM 2014; 370:734-43 Cisplatin 50 mg/m2 (d1 or d2) Paclitaxel 135 or 175 mg/m2 Open: 06-APR-09 Closed: 03-JAN-12 Accrual: 427 (eligible) I II +/- Bevacizumab 15 mg/kg Paclitaxel 175 mg/m2 (3 h) Topotecan 0.75 mg/m2 (d1,2,3) III IV +/- Bevacizumab 15 mg/kg
DSMB Review JAN-2012: No evidence of superiority for non-Cisplatin regimen Bifactorial Randomization 1. Chemotherapy 2. Bevacizumab
GCIG Education Symposium, November 2017, Vienna
Tewari KS, et al. NEJM 2014; 370:734-43
0.0 0.2 0.4 0.6 0.8 1.0 12 24 36 Months on Study
Progression-Free Survival
0.0 0.2 0.4 0.6 0.8 1.0 12 24 36 Months on Study
Overall Survival
Chemo + Bev (n = 227) Chemo + Bev (n = 227) Chemo Alone (n = 225) Chemo Alone (n = 225)
HR (+/- 97% CI) = 0.71 (0.54-0.95) p = 0.0035 (1-sided) Median: 17.0 vs 13.3 months HR (+/- 95% CI) = 0.67 (0.54-0.82) p = 0.0002 (2-sided) Median: 8.2 vs 5.9 months
FDA approved indication for bevacizumab with chemotherapy 14-AUG-2014
GCIG Education Symposium, November 2017, Vienna
Willmott LJ, et al. IGCS 2015
GCIG Education Symposium, November 2017, Vienna
Modified from: Advaxis Immunotherapies
Lm-LLOis phagocytosed by APC Some Lm-LLO escapes the phagolysosome and enters the cytosol Proteasomal degradation of tLLO-TAA fusion protein into peptides for MHC class I Ag presentation Some Lm-LLO is killed and degraded within the phagolysosome Peptide-MHC APC complexes stimulate CD4+ (MHC II) and CD8+ (MHC I) T cells
Lm, Listeria monocytogenes TAA, tumor-associated antigen tLLO, truncated listeriolysin O AXAL, Axalimogene Filolisbac
GCIG Education Symposium, November 2017, Vienna
Herzog T. for GOG-Foundation GOG-3009 (Advaxis ADXS001-02) Open: 03FEB2017 Target: 450 patients
GCIG Education Symposium, November 2017, Vienna
KEYNOTE-028 (NCT02054806) Phase IB Multicohort Frenel J-S, ASCO 2016 Total n = 24, Squamous n = 23
GCIG Education Symposium, November 2017, Vienna
GOG Foundation (under development)
therapy (platinum-refractory)
Open: SEP2017 Accrual: 436 pts
* Pemetrexed, topotecan, irinotecan, Vinorelbine, gemcitabine
GCIG Education Symposium, November 2017, Vienna
emphasis on high-risk populations in the developing world
(SHAPE)
chemotherapy, dose/schedule of cisplatin
chemotherapy for metastatic or recurrent disease, but with an increased risk
GCIG Education Symposium, November 2017, Vienna
Source: CDC Behavioral Risk Factor Surveillance System
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
GCIG Education Symposium, November 2017, Vienna
Schuler KM, et al. SGO 2014 (Abstract 8) IHC Molecular Markers (Pre- and Post-Rx) pAMPK 60.3% pAKT 44.2% pS6 51.2% p4EBP1 74.7% ER 65.7% PR (NC)
Mean Ki-67 Index Pre-Rx: 39.5 Post-Rx: 27.7 (n = 20) Pre-Rx Post-Rx
New Diagnosis BMI ≥30 Endometrioid Histology Metformin 850 mg QD Definitive Surgery (within 7-28 d)
GCIG Education Symposium, November 2017, Vienna
Bae-Jump V for NRG Carboplatin AUC 5 Paclitaxel 175 mg/m2 (3 h) Placebo (QDBID) R I II Carboplatin AUC 5 Paclitaxel 175 mg/m2 (3 h) Metformin 850 mg (QDBID) Metformin 850 mg BID Placebo BID Q21d x 6 cycles Maintenance (CR, PR, SD)
Open: 17-Mar-2014 Closed: (ongoing) Target: 540 pts (Phase II + III) Integrated Phase II (PFS) Phase III (OS) 240 pts phase II (60 events, PFS HR 0.76) 540 pts phase III (OS HR 0.76)
GCIG Education Symposium, November 2017, Vienna
Median Age 50 - 60 60 - 70 Estrogen Related Common Uncommon Obesity Common Variable Background Hyperplastic Atrophic Precursor EIN EGD, EIC Histology Endometrioid Serous, Clear Cell Molecular Alterations MLH/MSI, PTEN, K- RAS, FGFR2, - Catenin p53, 17p del, HER2/neu Detection Early-Stage Advanced-Stage Familial Risk HNPCC BRCA (serous) Spread LN, Distal LN, Peritoneal
GCIG Education Symposium, November 2017, Vienna
Billingsley CC, et al. SGO 2015 No Abnormality Sporadic Defect Probable Mutation MMR IHC Staining MLH1 Methylation MSI Testing Intact Methylated Negative MLH1 Loss Methylated Positive Some MMR Loss non-Methylated Positive Molecular Risk Low Low High Total N (%) 578 (62%) 253 (27%) 107 (11%) Family Hx N (%) 52/578 (9%) 26/253 (10%) 21/107 (20%) A Molecular Staging Study of Endometrial Carcinoma (PI: WT Creasman)
Recommend adoption of universal molecular tumor screening: IHC and methylation MSI testing Genomic Validation
GCIG Education Symposium, November 2017, Vienna
TCGA Network. Nature 497:67-73, 2013
POLE UltraMutated MSI Hypermutated Copy-Number Low Copy-Number High
GCIG Education Symposium, November 2017, Vienna
Le DT, et al. N Engl J Med 2015;372:2509-20
Colorectal: MMR Deficient = 11, MMR Proficient = 21 Non-Colorectal: MMR Deficient = 9 (endometrial = 2)
GCIG Education Symposium, November 2017, Vienna
Byron SA, et al. PLoS ONE 7: e30801, 2012 FGFR2
FGFR2, and PIK3CA
activity with VEGFR2
GCIG Education Symposium, November 2017, Vienna
Randall ME, et al. ASTRO 2017
Open: MAR-2009 Closed: FEB-2013 Target: 527 pts (eligible/treated)
and PA LN failure more common in VCB/C (9% at 5 y vs 4%, HR 0.47)
Pelvic RT (Median 45 Gy) 3D Conformal or IMRT +/- Brachytherapy Boost Brachytherapy (HDR or LDR) Carboplatin AUC=6 Paclitaxel 175 mg/m2 q3w (x3 cycles)
GCIG Education Symposium, November 2017, Vienna
Randall ME, et al. ASTRO 2017
Cumulative Incidence Pelvic or PA LN Recurrence
GCIG Education Symposium, November 2017, Vienna
Randall ME, et al. ASTRO 2017
GCIG Education Symposium, November 2017, Vienna
hypermutated subtypes, especially MSI-high
address drug resistance and the DNA damage response
minimally invasive surgery, well-tolerated chemotherapy (carboplatin-paclitaxel), and precision radiation therapy (3D conformal and IMRT)
yet been established
GCIG Education Symposium, November 2017, Vienna
Cisplatin Paclitaxel Cytoreduction IP Cisplatin NACT Bevacizumab
GCIG Education Symposium, November 2017, Vienna
13q14 (RB1)
GCIG Education Symposium, November 2017, Vienna
GCIG Education Symposium, November 2017, Vienna
Meyer L, et al. J Clin Oncol 34:3854-3863, 2016 Stage III-C Stage IV Within NCCN, NACT use increased from 16% to 34% in stage IIIC (P trend < .001), and from 41% to 62% in stage IV (P trend < .001)
GCIG Education Symposium, November 2017, Vienna
Hamilton CA, et al. Gynecol Oncol 122:521-6, 2011
Upper abdominal tumor burden correlated with inferior long-term clinical
GCIG Education Symposium, November 2017, Vienna
Horowitz NS, et al. J Clin Oncol 10.1200/JCO.2014.56.3106 Data from GOG0182 FIGO Stage III-IV (n = 2,655) Analyzed according to R0 (microscopic) or MR (macroscopic) residual, and pre-operative DS (disease score)
GCIG Education Symposium, November 2017, Vienna
From: Larue and Bellacosa. Oncogene 24:7443–7454, 2005
SCC15 AKT Activated E-cadherin Vimentin
GCIG Education Symposium, November 2017, Vienna
Reister M, et al. J Natl Cancer Inst 2014;106 doi:10.1093/jnci/dju048
Expression: Suboptimal Optimal Prognosis
associated with invasive metastatic behavior and suboptimal outcomes
surgical management
GCIG Education Symposium, November 2017, Vienna
Mahner S, Elser G, Fotopoulou C, et al. for TRUST
C P C P C P C P C P C P C P C P C P C P C P C P
Bevacizumab 15mg/sq x 15
Bevacizumab 15mg/sq x 15 S surgery C P Carboplatin AUC5 Paclitaxel 175 mg/sq
Site Qualification Accrual Status: 120/700 (May2017)
GCIG Education Symposium, November 2017, Vienna
Bregar A and Fleming G for NRG Oncology
Status: Concept in planning Target: Approximately 150 pts Notes: Evaluating options for NCI support (DCP or CTEP) CP (x3) CT-MRD Core Bx CP = Carboplatin AUC 6 (D1), Paclitaxel 80 mg/m2 (D1,8,15) CT-MRD = CT post-chemotherapy with minimal residual disease ICS = Interval Cytoreductive Surgery (minimally invasive allowed) CP (x3) ICS CP (x3) No ICS R
GCIG Education Symposium, November 2017, Vienna
Burger R, for NRG Oncology
Open: OCT 2016 Status: Ongoing Accrual (Phase I) Target: Approximately 150 pts CP (x3) ICS CP (x3) Observation CP (x3) + Rux CP (x3) + Rux Rux Maint (optional) ICS Core Bx R 1:2 CP = Carboplatin AUC 5 or 6 (D1), Paclitaxel 80 mg/m2 (D1,8,15) Rux = Ruxolitinib 10-15 mg PO BID (pending Phase 1) ICS = Interval Cytoreductive Surgery
GCIG Education Symposium, November 2017, Vienna
Yamada D, for NRG Oncology and U Chicago SPORE
Open: JUN 2014 Status: Ongoing Accrual (U Chicago SPORE) Target: 76 pts CP (x3) ICS CP (x3) Observation CP (x3) + MET CP (x3) + MET MET Maint ICS Core Bx R 1:2
CP = Carboplatin AUC 6 (D1), Paclitaxel 80 mg/m2 (D1,8,15) MET = Metformin 850 mg PO BID ICS = Interval Cytoreductive Surgery
GCIG Education Symposium, November 2017, Vienna
Chhatrapati Shivaji Terminus, Mumbai 2012
GCIG Education Symposium, November 2017, Vienna
Walker J. for GOG, SGO 2016 Carboplatin AUC=6 (IV) Paclitaxel 80 mg/m2 IV (d1,8,15) Bevacizumab (C2-6) Cisplatin 75 mg/m2 (IP) Paclitaxel 135 mg/m2 (d1, 3h) Paclitaxel 60 mg/m2 (d8, IP) Bevacizumab (C2-6) R I III II Carboplatin AUC=6 (IP) Paclitaxel 80 mg/m2 (d1,8,15) Bevacizumab (C2-6) Bevacizumab q21d x 16 Bevacizumab q21d x 16 Bevacizumab q21d x 16
Open: 27-Jun-2009 Closed: 29-Oct-2011 Accrual: 1560 pts (max 250 suboptimal)
GCIG Education Symposium, November 2017, Vienna
Walker J. for GOG, 2016
GCIG Education Symposium, November 2017, Vienna
Walker J. for GOG, 2016
effective as modified IP chemotherapy
GCIG Education Symposium, November 2017, Vienna
Fujiwara K, for GOTIC and JGOG
tube cancer (including suboptimal cytoreduction)
Paclitaxel 80 mg/m2/1h IV, weekly, Cycles 1-6 Carboplatin AUC 6 IV, Day 1, Cycles 1-6 Paclitaxel 80 mg/m2/1h IV, weekly, Cycles 1-6 Carboplatin AUC 6 IP, Day 1, Cycles 1-6
R
Target: 655 pts (closed OCT2016)
GCIG Education Symposium, November 2017, Vienna
GCIG Education Symposium, November 2017, Vienna
Chan JK, et al. NEJM, 2016
Carboplatin AUC=6 Paclitaxel 80 mg/m2 (d1,8,15) +/- Bevacizumab (C2-6)$ I II Bevacizumab q21d$ Bevacizumab q21d$ Carboplatin AUC=6 Paclitaxel 175 mg/m2 (d1) +/- Bevacizumab (C2-6) $
$ Use of Bevacizumab elected prior to randomization
R Open: 27-SEP-2010 Closed: 08-FEB-2012 (ACRIN JUN-2013) Target: 692 pts (randomized)
GCIG Education Symposium, November 2017, Vienna
Chan JK, et al. NEJM, 2016
Schedule ( n ) PFS (+) BEV Three-Weekly Dose-Dense Weekly 289 291 14.7 14.9 (-) BEV Three-Weekly Dose-Dense Weekly 57 55 10.3 14.2
paclitaxel was associated with improved PFS
bevacizumab in three-weekly therapy
GCIG Education Symposium, November 2017, Vienna
Ng C, et al. Clin Cancer Res 2017
GCIG Education Symposium, November 2017, Vienna
Ng C, et al. Clin Cancer Res 2017
Blood Flow Decreased Blood Flow Increased
GCIG Education Symposium, November 2017, Vienna
Clamp A, et al. ESMO 2017 IPS IPS Chemo x6 DPS Bx Chemo x3 DPS Chemo x3
ASSIGNED (Non-Randomized) RANDOMIZE
1:1:1 Carboplatin AUC=5 q3w Paclitaxel 175 mg/m2 q3w
1
Carboplatin AUC=5 q3w Paclitaxel 80 mg/m2 q1w
2
Carboplatin AUC=2 q1w Paclitaxel 80 mg/m2 q1w
3
Open: JUN-2011 Closed: NOV-2014 Target: 1566 pts
GCIG Education Symposium, November 2017, Vienna
Clamp A, et al. ESMO 2017
Arm 1 Arm 2 Arm 3 Standard Weekly paclitaxel Weekly carbo- paclitaxel Total Patients N=522 N=523 N=521 Progressions 330 (63%) 335 (64%) 338 (65%) Median PFS 17.9 months 20.6 months 21.1 months Log rank (vs Arm1) p=0.45 p=0.56 HR vs Arm 1 (97.5% CI) 0.92 (0.77, 1.09) 0.94 (0.79, 1.12) Restricted means 24.4 months 24.9 months 25.3 months
Primary Analysis PFS (ITT)
GCIG Education Symposium, November 2017, Vienna
Clamp A, et al. ESMO 2017
GCIG Education Symposium, November 2017, Vienna
Coleman R, for GOG Foundation
x 6 II Veliparib 400 mg PO BID Paclitaxel (standard or dose-dense) Carboplatin AUC 6 (IV)* Veliparib 150 mg PO BID x 6 I Paclitaxel (standard or dose-dense) Carboplatin AUC 6 (IV)* Placebo PO BID Placebo PO BID x 6 II Placebo PO BID Paclitaxel (standard or dose-dense) Carboplatin AUC 6 (IV)* Veliparib 150 mg PO BID
Collaborative development with AbbVie (M13-694) including international participation, seeking EMA and FDA regulatory approval Open: JUL 2015 Closed: MAY 2017 Target: ~1100 pts (264 BRCA1/2 +)
GCIG Education Symposium, November 2017, Vienna
immediate impact on regulatory approvals and PARPi utilization
and sequence has not been addressed in any prospective clinical trial…
normal CA125 and imaging (+/- secondary cytoreduction), and many patients could actually receive ineffective therapy for a prolonged period of time
symptomatic recurrence, and time off-therapy (in a non-curative setting)
establish optimal clinical benefit
as TFST, TSST, etc.
potentially limiting subsequent therapeutic benefit
GCIG Education Symposium, November 2017, Vienna
Moore K and Pignata S, for GOG-F and ENGOT YO39523/GOG-3015/ENGOT-ov39
Open: MAR 2017 Status: Ongoing Accrual Target: 1300 pts Carboplatin AUC=6 D1 Paclitaxel 175 mg/m2 D1 Bevacizumab 15 mg/kg D1 Atezolizumab 800 mg D1 R Carboplatin AUC=6 D1 Paclitaxel 175 mg/m2 D1 Bevacizumab 15 mg/kg D1 Placebo IV D1 I II Bevacizumab 15 mg/kg Placebo (q3w x 16 cycles) Bevacizumab 15 mg/kg D1 Atezolizumab 800 mg D1 (q3w x 16 cycles)
GCIG Education Symposium, November 2017, Vienna
O’Cearbhaill RE, for NRG Oncology
Open: MAY 2017 Status: Ongoing safety lead-in (Phase I Working Group) Target: 272 Phase II, Cumulative 488 Phase III PLD 40 mg/m2 IV q4w Bevacizumab 10 mg/kg IV q2w Atezolizumab 800 mg IV q2w PLD 40 mg/m2 IV q4w Bevacizumab 10 mg/kg IV q2w R PLD 40 mg/m2 IV q4w Atezolizumab 800 mg IV q2w I II III HR PFS ≤ 0.783 (88% power) HR OS* ≤ 0.625 (90% power) *one-tail α 0.0115 (multiple comparisons)
GCIG Education Symposium, November 2017, Vienna
Liu J, for NRG Oncology
Cediranib 30 mg QD Olaparib 200 mg BID Platinum-based combo* (IV) R *Carboplatin + gemcitabine or paclitaxel or PLD Olaparib 300 mg BID
Open: FEB 2016 Status: Ongoing Accrual Target: 550 pts (135 BRCA1/2 +)
GCIG Education Symposium, November 2017, Vienna
Adams S, for NRG Oncology Preliminary data from pilot clinical trial at U New Mexico (INST1419)
Potential Mechanisms:
murine tumor model with BRCA1m OvCa
increased expression of MHC1 and Fas
marker (exploratory endpoint)
Olaparib 300mg PO twice daily. Tremelimumab IV 10mg/kg monthly x6 then every 3 m, up to 2 years
GCIG Education Symposium, November 2017, Vienna
Adams S and Brady M, for NRG Oncology
Status: Concept in planning Target: 420 pts (126 BRCAm+, 168 HRD+, 126 HRD-)
GCIG Education Symposium, November 2017, Vienna
Monk BJ, et al. IGCS 2016 A0502 CA4P (VDA)
Study Complete
CA4P + Bev + PCC n=178 Bev + PCC n=178
ORR Data, PFS Data ORR Data Trigger Part 2 Trigger Part 2
Bev + PCC n=40 CA4P + Bev + PCC n=40
Untreated 1d CA4P 3d CA4P Phase II/III trial extending experience from GOG0186I
GCIG Education Symposium, November 2017, Vienna
Moore K, et al. for GOG Foundation
with a cleavable disulfide linker and the cytotoxic maytansinoid DM4
* Paclitaxel, PLD, or topotecan 2 : 1
GCIG Education Symposium, November 2017, Vienna
GOG Foundation I II BAY94-9343 6.5 mg/kg q3w PLD 30 mg/m2 q3w BAY94-9343 6.5 mg/kg q3w III PLD 50 mg/m2 q4w R
GCIG Education Symposium, November 2017, Vienna
advances in treatment and supportive care, with improved PFS-OS
(TRUST), but may have limited impact in patients with high disease burden
chemotherapy with either cisplatin or carboplatin
data from randomized trials are conflicting
questions about patient selection, timing, resistance, and combinations with
complicated by multiple pathways of immunosuppression
agents (VDA), and agents that target the DNA damage response
GCIG Education Symposium, November 2017, Vienna