
SLIDE 1
Overview of Sleep Disorders
Richard J. Schwab, M.D. Professor of Medicine Division of Sleep Medicine Pulmonary, Allergy and Critical Care Division University of Pennsylvania Medical Center Philadelphia, Pennsylvania
Overview of Sleep Disorders - Disclosures
- NIH grants - RO1/PPG (Obesity and OSA)
- Consultant:
– Apnicure – Foramis
Overview of Sleep Disorders
- Sleep deprivation:
– Normals/driving/Maggie’s law
- Sleep disorders causing daytime sleepiness:
– Restless leg syndrome/periodic limb movements – Narcolepsy - use of Provigil/Nuvigil/Xyrem – Parasomnias/REM behavior disorder – Insomnia - should we be using hypnotics?
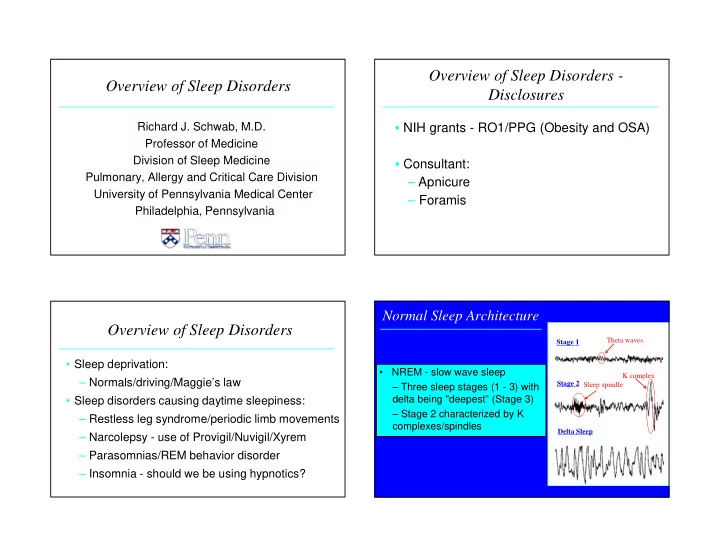
- NREM - slow wave sleep
– Three sleep stages (1 - 3) with delta being "deepest” (Stage 3) – Stage 2 characterized by K complexes/spindles
Normal Sleep Architecture
Stage 1 Stage 2 Delta Sleep Theta waves K complex Sleep spindle